
Left Ventricular Outflow Tract Obstruction (LVOTO) and SAM
- Michael Ritchie
- Oct 10, 2022
- 6 min read
What if I told you there is a cardiac disease process where you should give plenty of fluid and may have to start phenylephrine? It is not often that the answer to a cardiac disease question is to give more fluid, and phenylephrine has very little place in cardiac medicine. phenylephrine does not do a lot of things that benefit the heart and does a lot of things that are detrimental to the heart. It increases systemic afterload and increases wall tension in the LV. It is often mistakenly given in patients with LV disease and atrial fibrillation with RVR. It usually just prolongs afib with RVR and makes the LV work harder. It also increases pulmonary pressures and will make the right heart have to push against higher pressures which will lead to increased wall stress and more work on the RV. The is no place for phenylephrine in patients with pulmonary hypertension or RV dysfunction.
So where do fluid and phenylephrine have a place in cardiac intensive care medicine?
Left Ventricular Outflow Tract Obstruction
The left ventricular outflow tract is made up of the area between the mitral valve and the septal wall of the left ventricle.
Figure 1: Left Ventricular Outflow Tract

Left ventricular outflow obstruction (LVOTO) is a broad term though, and causes can fall outside of this defined area. When describing LVOTO, a lot of time is spent on congenital abnormalities. The congenital abnormalities are broken down by their location.
Table 1: Congenital LVOT Obstruction Categories:

Clinically, the most commonly encountered cause is hypertrophic cardiomyopathy which leads to systolic anterior motion of the mitral valve (SAM) and LVOTO. In the ICU these should be considered in hemodynamically compromised patients not responding to conventionally therapy.
LVOTO in the ICU
1. Hypertrophic Cardiomyopathy
2. Systolic Anterior Motion of the Mitral Valve (SAM)
Hypertrophic cardiomyopathy is the abnormal thickness of the left ventricular wall. This hypertrophy can be diffuse or septal.
Figure 2: Septal & Diffuse Hypertrophic Cardiomyopathy

Left ventricular outflow obstruction from hypertrophic cardiomyopathy is usually caused by SAM.
SAM is when the anterior leaflet of the mitral valve does not coapt with the posterior leaflet and is pulled over towards the intraventricular septum blocking the outflow tract. Also, because of the anterior leaflet being pulled over, it will cause mitral regurgitation.
Figure 3: Systolic Anterior Motion of the Mitral Valve (SAM)



SAM has a spectrum of severity and is often asymptomatic and found incidentally on echo. It is usually caused by hypertrophic cardiomyopathy but can be due to a number of causes.
Causes of SAM:
1. Hypertrophic cardiomyopathy
2. Catecholamine/Inotrope administration
3. Catecholamine surge
3. Acute myocardial infarction
4. Post mitral valve repair
5. Post aortic valve repair
The Physiology of LVOTO:
When it is mild or moderate it causes a reduction in stroke volume and cardiac output, but not significant enough to cause symptoms of heart failure or shock. It does cause increased afterload as shown in Laplace’s equation, it increases the ventricular pressure (P) which increases wall stress. This increased afterload leads to a dilated LV, ventricular wall thinning, and remodeling which over time will lead to systolic dysfunction and heart failure.
Figure 4: Laplace’s Law of Afterload

With severe LVOTO, the outflow of the LV is reduced to a point that the cardiac output is reduced enough that it leads to decompensated heart failure/cardiogenic shock.
Physiology of SAM:
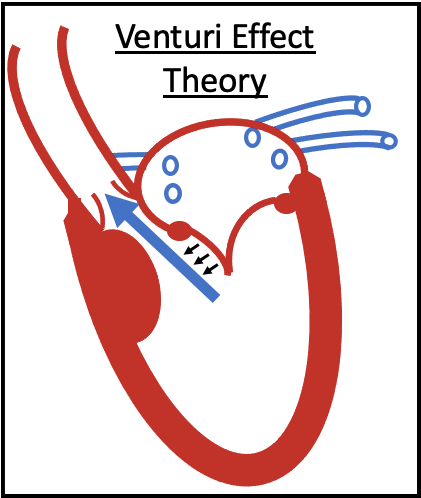
The physiology of SAM is up for debate. Since it was originally assumed that this only occurred with septal hypertrophy the theory was that the high velocity caused by the narrowing of the LVOT created lift and pulled the valve into the LVOT.
Figure 4: Venturi Effect Causing SAM
This does not fully explain SAM being seen in non-septal hypertrophy patients. It is likely multifactorial and requires abnormalities in the structure and the blood flow. Structurally, there is usually an anteriorly displaced papillary muscle or an increased length of the mitral valve leaflets. The blood inflow can be affected by these structural abnormalities depending on the loading conditions of the heart.
Ideally, the flow of blood through the mitral valve goes clockwise down the posterior wall to the apex and up the anterior wall, and to the LVOT.
Figure 5: Normal Ventricular Blood Flow

If this flow is altered, it can lead to LVOTO. When the mitral leaflets are long, or the papillary muscles are anterior, it leads to the blood inflow going towards the anterior wall and creates counterclockwise flow. When this occurs, the blood coming up the posterior wall leads to SAM and mitral regurgitation.
Figure 6: Blood Flow in SAM

Identifying LVOTO/SAM:
As stated before, this can only be seen on an echocardiogram. There are certain findings on echo that put people at risk for LVOTO and SAM. One of the main focuses on identifying people at risk is the distance between the intraventricular septum and mitral leaflet, which is often called the coapt/septal (CS) distance The closer this distance the higher the risk of LVOTO.
Anatomic findings:
1. Small LV cavity
2. Excess mitral leaflet tissue
3. Anteriorly displaced papillary muscles
4. Septal Hypertrophy
5. Decreased coapt/septal (CS) distance
Physiological findings:
1. LV hypovolemia
2. LV hypercontractility
3. Diastolic dysfunction
Diagnosing LVOTO:
Diagnosis of LVOTO requires the measurement of the peak gradient through the left ventricular outflow tract. If the gradient is ≥ 30 mmHg, LVOTO is diagnosed. If the gradient is ≥ 50 mmHg it is likely hemodynamically significant.
Medical Management of LVOTO/SAM:
Mild to moderate LVOTO/SAM can be medically managed, but severe LVOTO/SAM causes low cardiac output and shock and require the ICU.
Understanding the medical management of these patients is important since mechanical support devices are not helpful and emergent surgery is not typically performed. When a patient has had a cardiac arrest or is in a low cardiac output state due to this, it can be tempting to start them on inotropes to increase squeeze. This will actually make things worse and be detrimental to the patient.
If we look at the physiology discussed above, the problems are the distance between the mitral valve and the septum and the velocity through the outflow tract. Therefore, the treatment should target both issues.
1. Volume loading:
This is an important component of the treatment of LVOTO. Increasing the volume in the LV allows increased separation of the valve and intraventricular septum. It is important to make sure not to fluid overload them since they are also prone to pulmonary edema due to mitral regurgitation.
2. Rate reduction/Negative inotropy:
Beta blockers are the first line of treatment. It does two things that help with medical management. By decreasing the rate, it increases filling time which increases LV volume. Additionally, it is a negative inotrope which will decrease the velocity through the outflow tract.
Calcium channel blockers can be used if unable to take beta blockers or as an adjunct to patients refractory to beta blockers but must be non-dihydropyridine.
3. Increasing afterload:
Phenylephrine or vasopressin will increase systemic pressure which will increase afterload. The increased systemic pressure increases the wall tension which will lead to increased LV filling. Also, the increased pressure to push against will decrease the velocity.
LVOTO and SAM can be challenging to diagnose as it requires an echo to visualize the leaflet of the mitral valve within the tract or measure increased velocities within the LVOT. It is important to consider this in patients who are high risk or have unexplained shock or cardiac arrest.
As long as you remember the medical management, most patients can be supported until recovery or plan for surgery.
Figure 8: LVOTO/SAM Medical Management

Left Ventricular Heart Failure Series:
Part 1a: Introducing Preload
Part 1b: Measuring Preload
Part 2a: Physiological Contractility
Part 2b: Clinical Contractility
Part 3a: Simplifying Afterload
Part 3b: The Physiology of Afterload
Part 4: Managing LV dysfunction
Other Left Sided Heart Failure:
Part 1: Valvular disease
Part 2: LVOT obstruction/SAM
Cardiogenic Shock:
Part 1: Why a Protocol is Needed
Part 2: Cardiogenic Shock Protocols
References:
Manabe S, Kasegawa H, Arai H, Takanashi S. Management of systolic anterior motion of the mitral valve: a mechanism-based approach. Gen Thorac Cardiovasc Surg. 2018;66(7):379-389. doi:10.1007/s11748-018-0915-0
Vilcant V, Hai O. Left Ventricular Outflow Tract Obstruction. [Updated 2022 May 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470446/
Aboulhosn J, Child JS. Left ventricular outflow obstruction: subaortic stenosis, bicuspid aortic valve, supravalvar aortic stenosis, and coarctation of the aorta. Circulation. 2006;114(22):2412-2422. doi:10.1161/CIRCULATIONAHA.105.592089
Ibrahim M, Rao C, Ashrafian H, Chaudhry U, Darzi A, Athanasiou T. Modern management of systolic anterior motion of the mitral valve. Eur J Cardiothorac Surg. 2012;41(6):1260-1270. doi:10.1093/ejcts/ezr232
Park KS, Kim H, Jung YS, et al. Left ventricular outflow tract obstruction with systolic anterior motion of the mitral valve in patient with pericardial effusion caused by ascending aortic dissection -A case report-. Korean J Anesthesiol. 2013;64(1):73-76. doi:10.4097/kjae.2013.64.1.73



Comments